Unbeknownst to most there is constant influenza monitoring occurring globally. This allows us to estimate the strains most likely to circulate through human populations, develop vaccines targeted for the three most likely strains and simply prepare for annual influenza seasons. Prior to the culmination of candidate vaccine strains is monitoring animal populations where most, if not all influenza strains originate, mutate and become infectious to humans where additional mutations occur and so on. Some strains never make it into humans but many do.
One such influenza strain is being monitored in swine populations, H3N2 and its variant H3N2v has been infecting humans. Thus far, human infections have been reported in 8 states since July 2011, Hawaii, Illinois, Ohio, Iowa, Maine, Pennsylvania, Utah and West Virginia. All infected have had probable or definite exposure to infected swine however there have been three cases that were deemed as human to human transmitted. Although human-human transmission appears to be very limited, H3N2v does contain the M or matrix gene from the 2009 H1N1 influenza strain which may confer increased transmissibility to and between humans.
Since 90% and more pigs tested have been found to be infected with H3N2, the CDC is recommending that those who are vulnerable to influenza complications such as infants, young children, pregnant women, elderly and immune-compromised people avoid contact with pigs such as farms and fairs.
Thursday, August 9, 2012
Wednesday, August 8, 2012
Commercial vaccination provider told to stop misleading on their website
News is just in that Babyjabs.co.uk, the website of Dr Richard Halvorsen, a vaccine-critical GP, which promotes/sells single measles, (mumps) and rubella shots has been ordered by the Advertising Standards Authority to stop using misleading wording on their website. The Babyjabs website has been claiming
A quick look at the Babyjabs MMR web page today shows that there are still desperately promoting the MMR-autism link, citing the recent Italian MMR-ruling (Just the Vax passim), and emphasising MMR side effects, without comparing them to the complications of the disease (over 20% of measles patients in Merseyside were hospitalised). This is fear mongering at its best with the purpose of selling a part of the protection (mumps single vaccine has not been available in the UK for several years) that parents could get free on the NHS. Proponents of the single vaccines (often private doctors selling them) like to argue that offering parents the choice to get single vaccines will overall increase compliance and that they are just responding to parental requests. However, fact is that children on a selective schedule experience significant delays until full protection (if they are able to get all singles) and a sales site who meticulously lists all proven and alleged adverse vaccine events and concludes:
See also the excellent write up on Stuff and Nonsense who was the complainant...
"This means that the vaccine could be causing autism in up to 10% of autistic children in the UK - between 300 and 400 children a year. The vaccine strain measles virus has been found in the guts - and brains - of some autistic children; this research supports many parents' beliefs that the MMR vaccine has caused autism in their children".The complaint claimed:
1. the claim "Most experts now agree that the large rise [in autism] has been caused partly by increased diagnosis, but also by a real increase in the number of children with autism" was misleading and could be substantiated.and three points of the complaint were upheld by the ASA after review of Babyjabs' long response. Read the reasoning here - it is interesting.
2. the claim "the [MMR] vaccine could be causing autism in up to 10% of autistic children in the UK - between 300 and 400 children a year" was misleading and could be substantiated; and,
3. the claim "The vaccine strain measles virus has been found in the guts - and brains - of some autistic children; this supports many parents' belief that the MMR vaccine has caused autism in their children" was misleading and could be substantiated.
A quick look at the Babyjabs MMR web page today shows that there are still desperately promoting the MMR-autism link, citing the recent Italian MMR-ruling (Just the Vax passim), and emphasising MMR side effects, without comparing them to the complications of the disease (over 20% of measles patients in Merseyside were hospitalised). This is fear mongering at its best with the purpose of selling a part of the protection (mumps single vaccine has not been available in the UK for several years) that parents could get free on the NHS. Proponents of the single vaccines (often private doctors selling them) like to argue that offering parents the choice to get single vaccines will overall increase compliance and that they are just responding to parental requests. However, fact is that children on a selective schedule experience significant delays until full protection (if they are able to get all singles) and a sales site who meticulously lists all proven and alleged adverse vaccine events and concludes:
We do not offer the MMR vaccine at BabyJabs We are concerned that the safety of the vaccine has not been adequately demonstrated, and believe that the single vaccines are suitable alternatives that are equally – possibly more – effective and are probably safer.does not appear a "neutral provider" at all.
See also the excellent write up on Stuff and Nonsense who was the complainant...
Washington State Pertussis Outbreak
There is an outbreak of pertussis in Washington state that has produced a prevalence that hasn't been seen in decades. In fact, 1942 was the last time this many cases was recorded. So far there have been 3400 reported cases and the age groups most affected are infants less than one year old and children ages 10-13 years old. This outbreak, as in California two years ago has demonstrated the reduced duration of efficacy and to some extent, the overall efficacy of diphtheria, tetanus and acellular pertussis toxoid vaccines (DTaP). This has led to anti-vaxxers exploiting these outbreaks as a demonstration that DTaP vaccines are useless. Whereas nothing could be farther from the truth.
One particularly notorious anti-vaxxer, Joseph Mercola has used the California outbreak to triumphantly announce that the majority of those infected with pertussis were fully vaccinated. Well duh, the majority of children are fully vaccinated, but more on that later. He also cherry-picks an editorial that was published in Pediatrics written by eminent pertussis researcher J.D. Cherry earlier this year. Mercola only lists the contributing factors for the increase in pertussis prevalence and overestimation of vaccine efficacy but leaves out the contributing factors for underestimating vaccine efficacy and his conclusions. For instance, Dr. Cherry writes:
Another fallacy that Joe Mercola propagates along with his witless followers is that more vaccinated than unvaccinated have been infected with pertussis. When one simply looks at the raw data, it appears that way but those claiming more vaccinated than unvaccinated are being infected are either being wilfully dishonest, epidemiologically-ignorant or both. Let's look at the raw statistics from the CDC as of 20 July 2012 and the Washington Department of Health as of 4 August 2012 (in the format presented by Medical News Today):
As we can see, more un/undervaccinated children have been infected with pertussis than fully vaccinated across all age bins. This translates to children ages 5-9 un/der vaccinated children are 6 times more likely to become infected with pertussis than fully vaccinated. Children ages 10-13 un/der vaccinated are 25 times more likely to become infected with pertussis than fully vaccinated. And un/der vaccinated children ages 14-18 are 6 times more likely to become infected with pertussis than fully vaccinated.
Two hundred and fourteen infants under the age of one year were infected and 43 hospitalised. Twenty four percent of those three months to one year were un/undervaccinated. Of those hospitalised, 35 or 81% were three months or younger. This is appalling that these children suffered needlessly; we need to do more to protect this vulnerable population and people need to stop buying into anti-vaccine lies.
One particularly notorious anti-vaxxer, Joseph Mercola has used the California outbreak to triumphantly announce that the majority of those infected with pertussis were fully vaccinated. Well duh, the majority of children are fully vaccinated, but more on that later. He also cherry-picks an editorial that was published in Pediatrics written by eminent pertussis researcher J.D. Cherry earlier this year. Mercola only lists the contributing factors for the increase in pertussis prevalence and overestimation of vaccine efficacy but leaves out the contributing factors for underestimating vaccine efficacy and his conclusions. For instance, Dr. Cherry writes:
Of nasopharyngeal specimens from patients with cough illnesses sent to a commercial laboratory for PCR testing, during the 3-year period 2008–2010, it was found that 14% of the positive specimens were IS1001 positive, indicating B parapertussis infection.(14) In 2010, the positivity rate was 16.5%. These cases would appear as vaccine failures when they are not, as protection against B parapertussis is not expected from current pertussis vaccines.And:
Vaccine use has resulted in genetic changes in PT, PRN, and FIM in circulating B pertussis strains, and it has been suggested that this has led to increased vaccine failure rates.(22) At the present time, however, there is no evidence to support the hypothesis that evolution is allowing circulating B pertussis strains to escape from vaccine-produced antibodies.(23) If it were to occur, I would expect it to occur first in Denmark, where a PT toxoid vaccine has been in use for ∼15 years; this, as yet apparently has not happened.Given that Joe Mercola is a salesman, not a researcher and doesn't even know the difference between viruses and bacteria, I'm a bit more inclined to rely upon the expertise of a globally-recognised pertussis researcher who concludes:
To overcome the problem, it needs to be recognized that B pertussis is circulating in all age groups and, therefore, for herd immunity there is a need to universally vaccinate all age groups at frequent intervals.(24) New vaccines should be considered for development that include changes to enhance efficacy but retaining a low reactogenicity profile. This could be DTaP vaccines with multiple additional components and perhaps containing less PT. An alternative would be to develop DTP vaccines with detoxified lipopolysaccharide (the cause of reactions to whole-cell vaccines). It has also been suggested to develop “live vaccines.”(25) There are data available (not presented here), however, that indicate that immunity from DTP vaccines is better than that after infection; therefore, I do not think “live vaccines” are a worthwhile approach. Clearly, additional investments and innovations in pertussis vaccine development are needed to remove pertussis from its position as the leading vaccine preventable disease in the United States.It is obvious from the California pertussis outbreak in 2010 and the current Washington state as well as the rest of the U.S. currently, that more effective and durable vaccines are needed, certainly not returning to the "good ol' days" of the pre-pertussis vaccine era that begot thousands of infant deaths annually.
Another fallacy that Joe Mercola propagates along with his witless followers is that more vaccinated than unvaccinated have been infected with pertussis. When one simply looks at the raw data, it appears that way but those claiming more vaccinated than unvaccinated are being infected are either being wilfully dishonest, epidemiologically-ignorant or both. Let's look at the raw statistics from the CDC as of 20 July 2012 and the Washington Department of Health as of 4 August 2012 (in the format presented by Medical News Today):
- There have been a total of 3,400 cases reported statewide through week 31, compared to 287 reported cases in 2011 during the same time period. That is a 1085% increase for the same time period.
- The overall incidence year to date is 50.5 pertussis cases per 100,000 Washington residents with a rate in infants under one year of age of 241.7 per 100,000. Two hundred and fourteen infants under one year of age were reported as having whooping cough and forty-three of them were hospitalized. Of those hospitalized, thirty-five (81%) were very young (three months of age or younger). Adolescents aged 10-13 years old also have a high incidence rate, 238.2 per 100,000, and comprise 24% of the total cases.
- 75.8% of patients aged from 3 months to 10 years were up-to-date with their childhood diphtheria and tetanus toxoids and acellular pertussis (DTaP) doses.
- 43.1% of patients aged 11 and 12 years and 77.2% of 13 to 19 year olds were up-to-date with their TDaP booster shots.
- 93.2% of children aged from 19 to 35 months had received three or more doses, while 81.9% had received four or more in 2010.
- No deaths caused by whooping cough have been reported.
Ages 5-9: (ARv) 500/411023 x 100 = 0.12%
(ARn) 159/21633 x 100 = 0.73%
Ages 10-13 (ARv) 356/329076 x 100 = 0.11%
(ARn) 469/17320 x 100 = 2.7%
Ages 14-18 (ARv) 477/431968 x 100 = 0.11%
(ARn) 141/22735 x 100 = 0.62%As we can see, more un/undervaccinated children have been infected with pertussis than fully vaccinated across all age bins. This translates to children ages 5-9 un/der vaccinated children are 6 times more likely to become infected with pertussis than fully vaccinated. Children ages 10-13 un/der vaccinated are 25 times more likely to become infected with pertussis than fully vaccinated. And un/der vaccinated children ages 14-18 are 6 times more likely to become infected with pertussis than fully vaccinated.
Two hundred and fourteen infants under the age of one year were infected and 43 hospitalised. Twenty four percent of those three months to one year were un/undervaccinated. Of those hospitalised, 35 or 81% were three months or younger. This is appalling that these children suffered needlessly; we need to do more to protect this vulnerable population and people need to stop buying into anti-vaccine lies.
Monday, August 6, 2012
♭♩ ♫ what a difference 5 weeks make... ♫ ♬
New Merseyside measles numbers were released Friday and there are now 414 laboratory confirmed cases of measles, plus 173 probably cases. Measles are contagious - so to reiterate from yesterday:
Older pupils, students and adults should check their vaccination records to ensure that they really have had two MMRs, children older than 13 and younger than 41 months could get their second MMR early during an outbreak to reduce the risk.
Consider getting your infant (between 6 and 12 months) vaccinated, if s/he is at "higher risk" (daycare) and there is an outbreak in the area - almost a quarter of cases in this outbreak were in the under one-year-olds, who are at particularly high risk of complications.
Anyone who intends to work/volunteer in the medical sector should have had two MMRs. In this, as in nearly every recent outbreak, transmissions within the medical setting and to medical personnel occurred.
Doctors and nurses need to familiarise themselves with the symptoms of measles, so that they can diagnose them early and limit transmission in the medical setting.
And finally, all parents need to think long and hard before taking their child into A&E or their GP's practice whether their child could be contagious, especially if the child has not had their MMRs and could be carrying a potentially fatal disease. Call ahead, get an "out of hours" appointment or home visit, if at all possible.
Edited to exchange first link to go to original source
Older pupils, students and adults should check their vaccination records to ensure that they really have had two MMRs, children older than 13 and younger than 41 months could get their second MMR early during an outbreak to reduce the risk.
Consider getting your infant (between 6 and 12 months) vaccinated, if s/he is at "higher risk" (daycare) and there is an outbreak in the area - almost a quarter of cases in this outbreak were in the under one-year-olds, who are at particularly high risk of complications.
Anyone who intends to work/volunteer in the medical sector should have had two MMRs. In this, as in nearly every recent outbreak, transmissions within the medical setting and to medical personnel occurred.
Doctors and nurses need to familiarise themselves with the symptoms of measles, so that they can diagnose them early and limit transmission in the medical setting.
And finally, all parents need to think long and hard before taking their child into A&E or their GP's practice whether their child could be contagious, especially if the child has not had their MMRs and could be carrying a potentially fatal disease. Call ahead, get an "out of hours" appointment or home visit, if at all possible.
Edited to exchange first link to go to original source
Sunday, August 5, 2012
Record measles outbreak in UK's Merseyside hits un- and undervaccinated
it is another bad year for measles - following on the European measles record year 2011, which saw, from January to October, 26'000 cases, with 9 deaths and nearly 7300 hospitalisation, measles are still going strong in UK. Various regions are reporting outbreaks, Wales saw over 100 cases in Gwynedd and Porthmadog. Sussex has seen just over 300 cases of measles this year. The area worst hit is Merseyside, a small county in England's North West, with a population just under 1.4 million. After a single measles case was seen in January, case numbers slowly increased to nearly 360 confirmed and over 150 suspected cases by the end of June. Luckily, there has not been a death so far, but 18% of the confirmed cases had to be hospitalised. Contrary to rumours circulating on the internet, the outbreak was not mostly in fully vaccinated children (it is interesting how pertussis and measles myths and facts mix and make for new vaccine-sceptical tales). The HPA team have now published the break down of measles numbers in this outbreak and of the proportion of vaccinated and unvaccinated patients. Indeed, only 12 of the 359 confirmed cases (3.3%) have had two MMRs*. The associated figure is very telling:
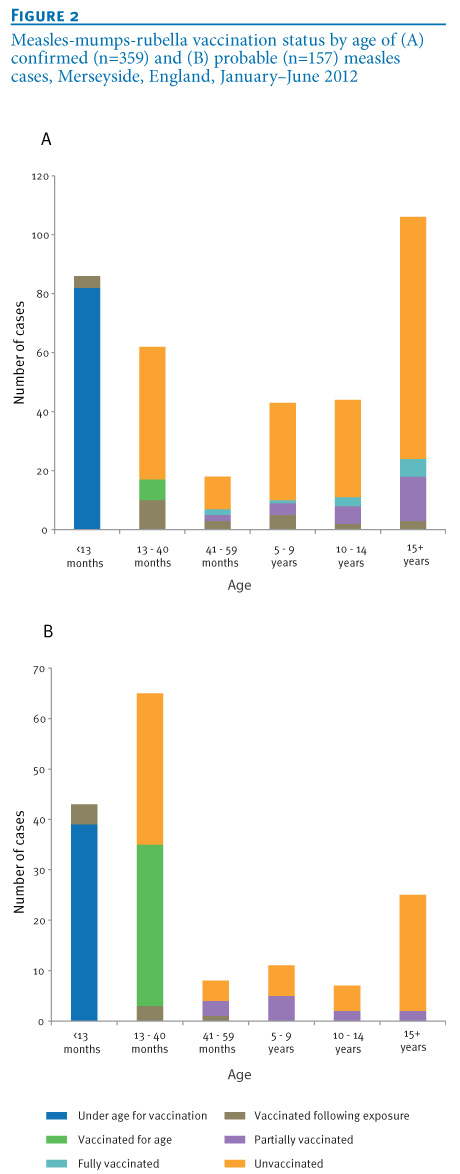 Take a good look at this. All orange and dark blue are unvaccinated, all green and purple are just vaccinated once (the UK recommends the first MMR at 13 months, the second at 41, so all green children were vaccinated age-appropriately only once). Only the light blue had 2x MMR. You may have to search for that stripe a bit, it is quite small. This is particularly interesting, since Merseyside has quite a high vaccine uptake, with 96% of children in Liverpool having had their first MMR. Consequently, the characteristics of this outbreak are very different from one in a largely unvaccinated population (like for example the 2008 outbreak in Salzburg, where 202 cases occurred in a month, largely in a 300 pupil Steiner school with 20% vaccine coverage), propagation of the measles is slow, with cases infecting very few other people. While it is a bit discouraging that the high vaccination coverage amongst young children has not stopped the outbreak entirely, it is clear what can be done.
Take a good look at this. All orange and dark blue are unvaccinated, all green and purple are just vaccinated once (the UK recommends the first MMR at 13 months, the second at 41, so all green children were vaccinated age-appropriately only once). Only the light blue had 2x MMR. You may have to search for that stripe a bit, it is quite small. This is particularly interesting, since Merseyside has quite a high vaccine uptake, with 96% of children in Liverpool having had their first MMR. Consequently, the characteristics of this outbreak are very different from one in a largely unvaccinated population (like for example the 2008 outbreak in Salzburg, where 202 cases occurred in a month, largely in a 300 pupil Steiner school with 20% vaccine coverage), propagation of the measles is slow, with cases infecting very few other people. While it is a bit discouraging that the high vaccination coverage amongst young children has not stopped the outbreak entirely, it is clear what can be done.
Coverage for the second MMR needs to be increased. Older pupils, students and adults should check their vaccination records to ensure that they really have had two MMRs, children older than 13 and younger than 41 months could get their second MMR early during an outbreak to reduce the risk.
Consider getting your infant (between 6 and 12 months) vaccinated, if s/he is at "higher risk" (daycare) and there is an outbreak in the area - almost a quarter of cases in this outbreak were in the under one-year-olds, who are at particularly high risk of complications.
Anyone who intends to work/volunteer in the medical sector should have had two MMRs. In this, as in nearly every recent outbreak, transmissions within the medical setting and to medical personnel occurred.
Doctors and nurses need to familiarise themselves with the symptoms of measles, so that they can diagnose them early and limit transmission in the medical setting.
And finally, all parents need to think long and hard before taking their child into A&E or their GP's practice whether their child could be contagious, especially if the child has not had their MMRs and could be carrying a potentially fatal disease. Call ahead, get an "out of hours" appointment or home visit, if at all possible.
* Footnote: instead of complaining about vague language in HPA reports and speculating about the number of fully vaccinated children in this outbreak, people could have just emailed/called the HPA. They do have a presence on Facebook, too and are quite happy to answer any question in depth (I have talked to them through FB, email and phone).
Coverage for the second MMR needs to be increased. Older pupils, students and adults should check their vaccination records to ensure that they really have had two MMRs, children older than 13 and younger than 41 months could get their second MMR early during an outbreak to reduce the risk.
Consider getting your infant (between 6 and 12 months) vaccinated, if s/he is at "higher risk" (daycare) and there is an outbreak in the area - almost a quarter of cases in this outbreak were in the under one-year-olds, who are at particularly high risk of complications.
Anyone who intends to work/volunteer in the medical sector should have had two MMRs. In this, as in nearly every recent outbreak, transmissions within the medical setting and to medical personnel occurred.
Doctors and nurses need to familiarise themselves with the symptoms of measles, so that they can diagnose them early and limit transmission in the medical setting.
And finally, all parents need to think long and hard before taking their child into A&E or their GP's practice whether their child could be contagious, especially if the child has not had their MMRs and could be carrying a potentially fatal disease. Call ahead, get an "out of hours" appointment or home visit, if at all possible.
* Footnote: instead of complaining about vague language in HPA reports and speculating about the number of fully vaccinated children in this outbreak, people could have just emailed/called the HPA. They do have a presence on Facebook, too and are quite happy to answer any question in depth (I have talked to them through FB, email and phone).
Saturday, August 4, 2012
Wakefied Defamation Suit Dismissed
Earlier this year, just shy of the statute of limitations, Andrew Wakefield launched a curious defamation lawsuit against the British Medical Journal (BMJ), journalist Brian Deer and the BMJ editor Fiona Godlee. His sad rump of disciples even set up a "Wakefield Justice Fund" so supporters could give Wakefield money to pursue the lawsuit. It was curious because Texas, where the suit was filed had just implemented a strong anti-SLAPP statute, Wakefield is a British citizen, the BMJ a British publication and Deer and Godlee also British citizens, and curious because Wakefield has tried to sue Brian Deer before but failed miserably.
Wakefield's defamation suit has been dismissed on jurisdictional grounds. Wakefield vows to appeal however:
Wakefield's defamation suit has been dismissed on jurisdictional grounds. Wakefield vows to appeal however:
Wakefield, who is 55 and lives in Austin, vowed to pursue it. “We think we have a very good argument, and we plan to appeal,” he said.The harm caused by Wakefield's fraud will never be fully undone. Although it is apparent that many have distanced themselves from him and if nothing else, Wakefield's antics provide copious blog fodder and a lesson to others.
Friday, August 3, 2012
100% certainty
Very few things are 100% certain in life and as a biomedical researcher, I am used to expressing things cautiously using phrases like "is consistent with", "there is no evidence for". However, of late, I have seen a claim that I can say with 100% certainty is not true.
My DS/DD caught pertussis from the vaccine (and iterations thereof, like "from the vaccine that a vaccinated child shed").
Not true. How do I know that?
Pertussis is a bacterial infection. Whole, living bacteria called Bordetella pertussis enter our nose/mouth because someone coughed them at us and they stick to the tiny little hairs (cilia) in our respiratory tract - here is a picture (source):

The bacteria have some proteins on the surface that help them hold on to those hairs and manipulate the immune response. In order to have a noticeable effect, the bacteria have to multiply, using loads of genes and proteins within their cell membrane (see below) and the nutrients provided by our body. Here is a picture of the bacteria (coloured from an electron micrograph in which they are 40.000x enlarged - source):

So why can't the vaccine cause pertussis? Because there are no bacteria in it. The vaccine only contains the surface bits that help the bacteria attach to those ciliated cells in your respiratory tract. For example, Daptacel contains:
10 µg detoxified pertussis toxin (PTx), 5 µg filamentous hemagglutinin (FHA), 3 µg pertactin (PRN), and 5 µg fimbriae types 2 and 3 (FIM) - I have circled them in red in the following picture (source):
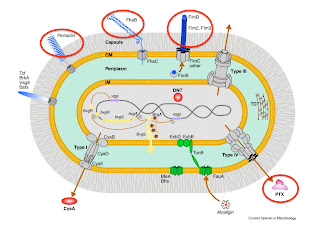
The idea is that in response to vaccination, the body generates antibodies only against those proteins - those will bind to the surface of the bacteria when someone coughs at you and prevent the bacteria from sticking to your respiratory tract. Everything that is not circled in red is NOT in the vaccine. There is no chance that some surface bits injected into your arm or leg cause an illness that requires loads of bacteria sticking to those tiny cilia in your respiratory tract. Furthermore, the vaccine also does not contain the tracheal cytotoxin, which the bacteria release and which paralyses those cilia and prevent them from clearing your airways, which is what causes the characteristic cough (<- click on that link - this is what pertussis sounds like).
100%
My DS/DD caught pertussis from the vaccine (and iterations thereof, like "from the vaccine that a vaccinated child shed").
Not true. How do I know that?
Pertussis is a bacterial infection. Whole, living bacteria called Bordetella pertussis enter our nose/mouth because someone coughed them at us and they stick to the tiny little hairs (cilia) in our respiratory tract - here is a picture (source):
The bacteria have some proteins on the surface that help them hold on to those hairs and manipulate the immune response. In order to have a noticeable effect, the bacteria have to multiply, using loads of genes and proteins within their cell membrane (see below) and the nutrients provided by our body. Here is a picture of the bacteria (coloured from an electron micrograph in which they are 40.000x enlarged - source):
So why can't the vaccine cause pertussis? Because there are no bacteria in it. The vaccine only contains the surface bits that help the bacteria attach to those ciliated cells in your respiratory tract. For example, Daptacel contains:
10 µg detoxified pertussis toxin (PTx), 5 µg filamentous hemagglutinin (FHA), 3 µg pertactin (PRN), and 5 µg fimbriae types 2 and 3 (FIM) - I have circled them in red in the following picture (source):

The idea is that in response to vaccination, the body generates antibodies only against those proteins - those will bind to the surface of the bacteria when someone coughs at you and prevent the bacteria from sticking to your respiratory tract. Everything that is not circled in red is NOT in the vaccine. There is no chance that some surface bits injected into your arm or leg cause an illness that requires loads of bacteria sticking to those tiny cilia in your respiratory tract. Furthermore, the vaccine also does not contain the tracheal cytotoxin, which the bacteria release and which paralyses those cilia and prevent them from clearing your airways, which is what causes the characteristic cough (<- click on that link - this is what pertussis sounds like).
100%
Subscribe to:
Posts (Atom)